
Owners often get very confused about when to allow a horse to return to movement following laminitis, and unfortunately incorrect and often dangerous advice can be found on the internet suggesting that horses with laminitis should be encouraged to move, without explaining when movement may be beneficial or harmful.

| This horse was encouraged to move - he was turned out in a large field with uncorrected rotation and was found dead with his pedal bones sticking out through his soles. Movement before the feet are correctly aligned and stable can cause (further) damage and rotation/sinking. | 
|
Movement is thought to be beneficial to healing, but only once the foot is mechanically correct, stable, supported, and the cause of the laminitis has been removed.
1. Active laminitis - no movement
During active endocrine laminitis, the laminae stretch and weaken, and the basement membrane may become damaged causing complete separation of the laminae (this may be more likely with SIRS laminitis). The connection of the hoof to the skeleton is unstable. Movement increases pressure on these damaged structures.
1. Active laminitis - no movement
During active endocrine laminitis, the laminae stretch and weaken, and the basement membrane may become damaged causing complete separation of the laminae (this may be more likely with SIRS laminitis). The connection of the hoof to the skeleton is unstable. Movement increases pressure on these damaged structures.
| During this time horses should be confined to prevent movement as much as possible, encouraged to lie down, with food and water close by and ideally above the ground to reduce pressure on the front feet. The area of confinement should have deep, soft, conforming and supportive bedding (e.g. sand, sawdust) which packs into the hollows of the foot to increase the weight bearing surface, particularly at the back of the foot where the horse will want to bear its weight, and/or pads fitted to relieve pressure on the less-than-well-connected walls and spread weight bearing over the less painful areas at the back of the foot. 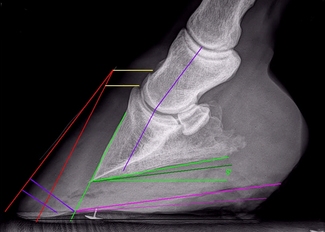
| 
The feet should be x-rayed ASAP and any rotation corrected with a realigning trim. This means the palmar angle should be between around 2 and 5 degrees and the dorsal angle should be returned to 0 by bevelling breakover at the toe (purple lines on x-ray suggest possible breakover positions), whilst retaining hoof wall above the bevel to provide strength and protection to the foot. The outer wall should be bevelled to minimise separating forces. |
A horse in pain from laminitis should not be forced to walk - pain tells a horse that he has damage and shouldn't move. NSAID (Bute, Danilon etc) use should be kept to a minimum, and should be discontinued at least 48 hours before a horse is encouraged to return to movement. Horses taking NSAIDs should be kept confined and discouraged from moving.
2. Post active laminitis and realignment - return to movement
Once
most horses can return to some free choice movement and controlled in-hand exercise.
Turnout should be in a small, safe, enclosed area with good footing, ideally soft and conforming such as sand, pea gravel, mud.
Taylor D, Sperandeo A, Schumacher J, Passler T, Wooldridge A, Bell R, Cooner A, Guidry L, Matz-Creel H, Ramey I, Ramey P
Clinical Outcome of 14 Obese, Laminitic Horses Managed with the Same Rehabilitation Protocol
JEVS published online 05 Feb 2014
gives this advice for returning to exercise:
"2.5. Management Protocol: Exercise
Turnout in a grass-free paddock or daily in-hand exercise was encouraged after the following (1) hooves had been trimmed to minimize weight bearing by the hoof wall; the desired heel plane and palmar angle (≤ 10* degrees) had been established by trimming; and when the hooves had been protected by soft protective hoof boots with pads (as described in Section 2.3) that provided enough comfort for the horse to have a heel-first hoof landing. In-hand exercise was increased daily by adding 5- to 10-minute increments to each exercise session until horses were walking 30 to 45 minutes 2 or 3 times daily. Owners were instructed to observe for the intended heel-first impact of the hoof boot and to walk the horse only while the hoof boots were securely in place. They were instructed not to walk the horse if the hoof impact appeared to be toe-first and to discontinue daily walking (and call the veterinary/hoof care provider team) if the horse seemed to have increasing pain after walking."
(* NB there is a mistake in the paper, corrected above - the palmar angle should be < or equal to 10 degrees, not 0 degrees - confirmed in personal correspondence with Debra Taylor).
2. Post active laminitis and realignment - return to movement
Once
- the cause of the laminitis has been diagnosed and removed/treated, and no further "active" laminitis is present;
- the feet have been realigned and balanced so that the palmar angle and breakover are correct;
- the feet are stable (i.e. there is no reason to expect further rotation/sinking, e.g. no gas pockets which might suggest total separation of the laminae);
- the feet are supported and protected with boots and thick pads to maximise weight bearing on the non-painful structures at the back of the foot and the horse is comfortably landing heel first; and
- the horse has been off NSAIDs/pain relief for at least 48 hours and is comfortable
most horses can return to some free choice movement and controlled in-hand exercise.
Turnout should be in a small, safe, enclosed area with good footing, ideally soft and conforming such as sand, pea gravel, mud.
Taylor D, Sperandeo A, Schumacher J, Passler T, Wooldridge A, Bell R, Cooner A, Guidry L, Matz-Creel H, Ramey I, Ramey P
Clinical Outcome of 14 Obese, Laminitic Horses Managed with the Same Rehabilitation Protocol
JEVS published online 05 Feb 2014
gives this advice for returning to exercise:
"2.5. Management Protocol: Exercise
Turnout in a grass-free paddock or daily in-hand exercise was encouraged after the following (1) hooves had been trimmed to minimize weight bearing by the hoof wall; the desired heel plane and palmar angle (≤ 10* degrees) had been established by trimming; and when the hooves had been protected by soft protective hoof boots with pads (as described in Section 2.3) that provided enough comfort for the horse to have a heel-first hoof landing. In-hand exercise was increased daily by adding 5- to 10-minute increments to each exercise session until horses were walking 30 to 45 minutes 2 or 3 times daily. Owners were instructed to observe for the intended heel-first impact of the hoof boot and to walk the horse only while the hoof boots were securely in place. They were instructed not to walk the horse if the hoof impact appeared to be toe-first and to discontinue daily walking (and call the veterinary/hoof care provider team) if the horse seemed to have increasing pain after walking."
(* NB there is a mistake in the paper, corrected above - the palmar angle should be < or equal to 10 degrees, not 0 degrees - confirmed in personal correspondence with Debra Taylor).

Further information: | Exactly when a horse should be encouraged to move, and eventually return to work following laminitis, will be individual to every case and depend on the extent of the damage to the feet, but in nearly all cases this advice regarding a return to movement will be appropriate: don't do it too soon, and don't leave it too long - get it right! 
|
Returning to work after laminitis - www.thelaminitissite.org
Hoof rehabilitation protocol - Debra Taylor, Ivy Ramey, Pete Ramey - www.hoofrehab.com
Taylor D, Sperandeo A, Schumacher J, Passler T, Wooldridge A, Bell R, Cooner A, Guidry L, Matz-Creel H, Ramey I, Ramey P
Clinical Outcome of 14 Obese, Laminitic Horses Managed with the Same Rehabilitation Protocol
JEVS published online 05 Feb 2014
DDT-Trim - www.ecirhorse.org
Hoof rehabilitation protocol - Debra Taylor, Ivy Ramey, Pete Ramey - www.hoofrehab.com
Taylor D, Sperandeo A, Schumacher J, Passler T, Wooldridge A, Bell R, Cooner A, Guidry L, Matz-Creel H, Ramey I, Ramey P
Clinical Outcome of 14 Obese, Laminitic Horses Managed with the Same Rehabilitation Protocol
JEVS published online 05 Feb 2014
DDT-Trim - www.ecirhorse.org
 RSS Feed
RSS Feed