
|
If you are looking for help because your horse has laminitis, EMS or PPID, please join Friends of TLS (FoTLS)
|
To support our rehabilitation & rescue work and to keep this website alive, please consider making a donation
|
LaminitisWhat is laminitis?
What causes laminitis? Symptoms of laminitis Symptoms of chronic laminitis - rotation/sinking Emergency treatment for laminitis Management of laminitis FAQs Further information - websites Further information - books and articles Laminitis Research |
|
What is laminitis?Download our Laminitis, EMS & PPID summary
Laminitis used to be defined as inflammation of the laminae, or lamellae (the laminae/lamellae are "velcro-like" connections between the pedal/coffin bone and the hoof) - "-itis" means inflammation. However, now we know that the majority of cases of laminitis have an endocrine cause, and there may be little or no inflammation involved in endocrine laminitis. Therefore laminitis may be defined as damage to or failure of the laminae, which may include stretching or separation of the laminae. Some vets suggest using the term "laminopathy" rather than laminitis. The laminae connections start to stretch, separate and break down, allowing the pedal/coffin bone and hoof capsule to rotate or sink in relation to each other - this rotation and/or sinking is called founder or chronic laminitis. Successful treatment is dependent on: 1. Recognising that the horse has laminitis. 2. Identifying and removing/treating the cause. 3. Supporting and realigning the feet as quickly as possible. With a positive diagnosis, appropriate treatment and management, and good foot care to fully realign any damage and then keep the foot correctly balanced, many horses return to their former use and live healthy long lives.
What causes laminitis?3 classes or causes of laminitis are currently recognised:
Endocrinopathic or insulin-related laminitis - due to hyperinsulinaemia/insulin dysregulation (ID) By far the most common cause of laminitis (around 90% of all laminitis cases), and most common in ponies and "good doer" breeds. Horses will have insulin dysregulation (ID), which can be due to Equine Metabolic Syndrome (a syndrome/collection of risk factors, not a disease, due to a combination of genetics and management). Horses with PPID can also have insulin dysregulation and an increased risk of laminitis. However, the link between PPID and laminitis is not understood, and it may be that some horses with PPID and laminitis have EMS and PPID. Pasture associated laminitis is endocrinopathic laminitis. Inflammatory or sepsis-related laminitis - "sick horse laminitis" This laminitis develops when a horse is already seriously ill with an inflammatory/septic illness, such as colitis, septicaemia, peritonitis, retained placenta, and potentially serious cases of carbohydrate/grain overload, such as if a horse breaks into a feed room. The horse will be systemically ill, will usually have a raised temperature and abnormal white blood cell counts and will often have diarrhoea and/or be depressed. Starch, fructan and black walnut shavings have all been used to induce sepsis-related laminitis experimentally. The primary illness must be treated. Icing the feet (cryotherapy) has been found to be very effective at halting the progression of laminitis in horses with a sepsis-related laminitis. More.. Supporting Limb Laminitis (SLL) - "lame horse laminitis" A severe protracted non-weightbearing lameness, e.g. a fracture or septic joint condition, can cause laminitis in another leg, usually the other leg in a pair. More.. Barbaro, winner of the 2006 Kentucky Derby, fractured his right hind and developed SLL 2 months later. He recovered, but a further operation led to laminitis in both front feet and he was put to sleep. The use of corticosteroids has also been implicated in causing or worsening laminitis, particularly in horses that are already prone to laminitis (therefore likely have an underlying, and possibly undetected, endocrinopathy). One injection of dexamethasone (20mg/500kg) caused insulin to increase from 166 to 844 IU in previously laminic ponies, 22 to 206 IU in normal ponies in July in ponies kept at pasture - Borer et al. 2010. Coleman M, Belknap J, Bramlage L, Eades S, Fraley B, Galantino-Homer H, Hunt R, Geor R, McCue M, McIlwraith W, Moore R, Peroni J, Townsend H, White N, Cummings K, Ivanek-Miojevic R, Cohen N Case Control Study of Pasture and Endocrinopathy-Associated Laminitis in Horses Equine Endocrinology Summit 2017 "Horses with an obese body condition (BCS ≥ 7), generalized or regional adiposity, a historic diagnosis of an endocrinopathy, and recent glucocorticoid administration were at increased odds of developing PEAL". Many causes of laminitis have been suggested, but currently only 5 causes have reliably induced laminitis experimentally: starch, black walnut, oligofructose, fructose and insulin: 80 Causes, predispositions, and pathways of laminitis Henry W. Heymering |
"What is Laminitis?" video - www.prascend.com
This video, created by Dr Andrew van Eps, of time-lapse x-rays shows the progression over 4 weeks of a sepsis-related laminitis due to Potomac Horse Fever. P3 rotation & sinking, separation of P3 from the dorsal hoof wall and decreasing sole depth are seen. The video was created by Dr Andrew van Eps, the horse was treated at Pennsylvania School of Veterinary Medicine.
Archived webinar from 25 April 2012:
Laminitis Lessons: A Webinar for Every Horse Owner - Don Walsh DVM from the Animal Health Foundation Equine Laminitis 2012 Update videos from the Animal Health Foundation
Laminitis definitions
Laminitis = damage to or failure of the laminae (inflammation is not significant in most cases of laminitis)
Founder = loss of normal orientation between the hoof capsule and the pedal bone, i.e. rotation or sinking Distal descent = sinking Laminae = lamellae Pedal bone = coffin bone = P3 = third phalanx 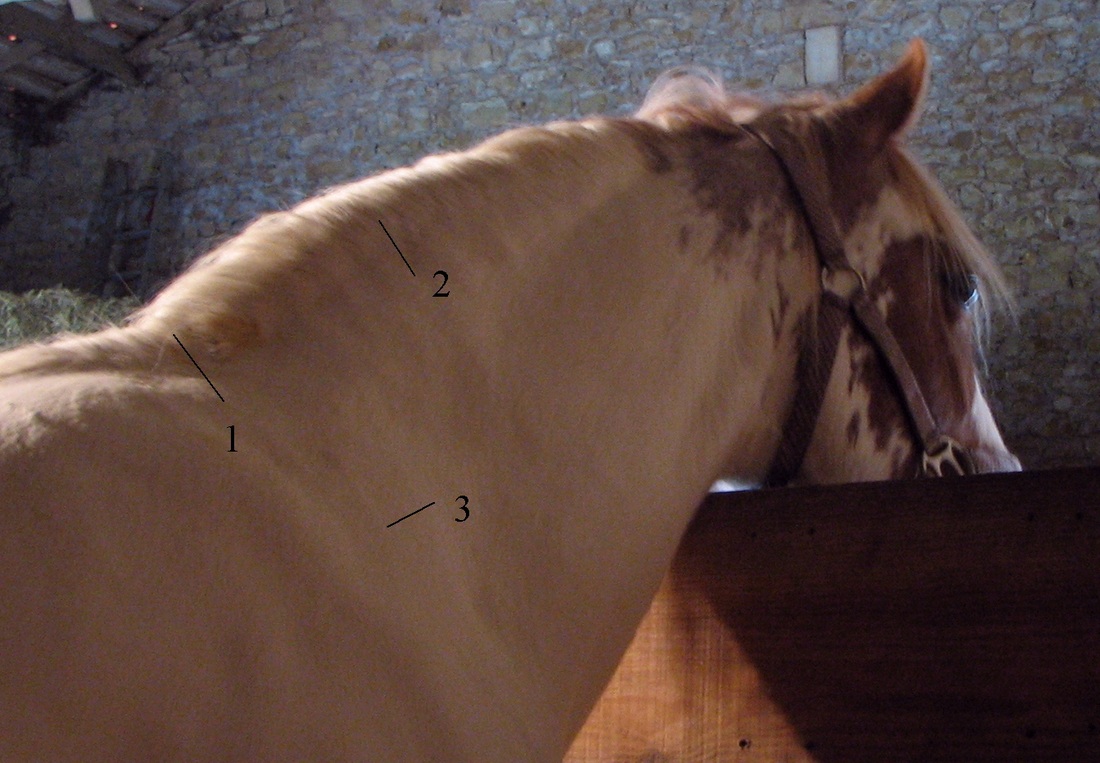
Signs of EMS: 1. dip as neck joins withers, 2. enlarged crest, often with "sausage-like" fat deposits, 3. lack of shoulder definition due to obesity.

An aged horse with PPID being cared for by Remus Memorial Horse Sanctuary. Advanced symptoms include long curly coat that isn't shed, weight loss and loss of top line, laminitis, recurrent infections, excess drinking and urination, depression and lethargy.
|



Symptoms of laminitisYou are unlikely to see all of these signs - consider laminitis (and call your vet) if you horse shows ANY of these symptoms, but be aware that many are also symptoms of other hoof/lameness issues. Perhaps the most reliable and one of the earliest signs is paddling - but a horse with sinking may not paddle. Symptoms will change as laminitis progresses from acute to chronic. Every horse is different and will show different symptoms and different degrees of pain - recognise and investigate any of these signs - too many horses go undiagnosed because the early signs of laminitis are not picked up - the earlier you recognise the symptoms, remove the cause and support the feet, the better the outcome is likely to be.
Horses with distal descent will be reluctant to move, have bounding digital pulses and have a depression at the coronet. They usually stand in a normal stance and may have abnormally cold feet. See Rosie's case study to see her symptoms of acute laminitis. 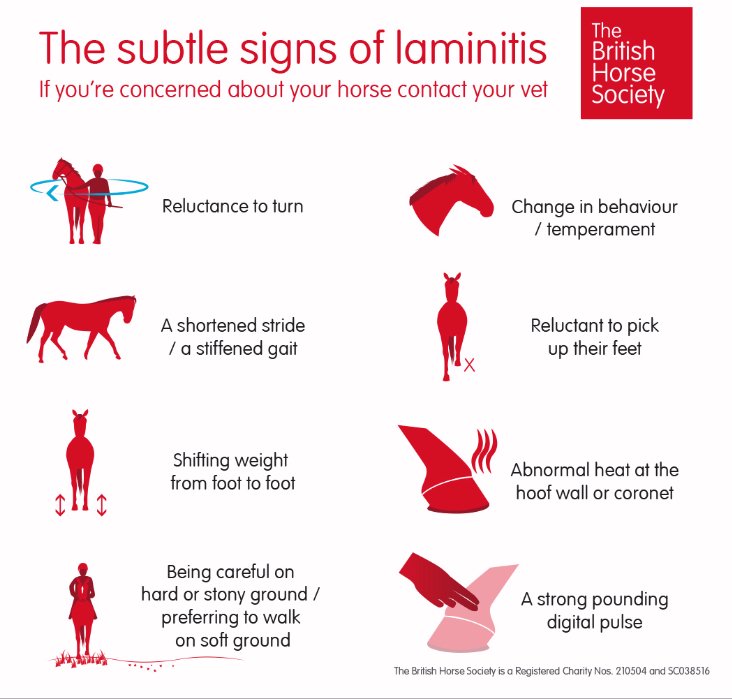
|

Abnormal stance

Bounding digital pulse - take at fetlock or pastern


Wall flare and bruising

Penetration of sole by P3
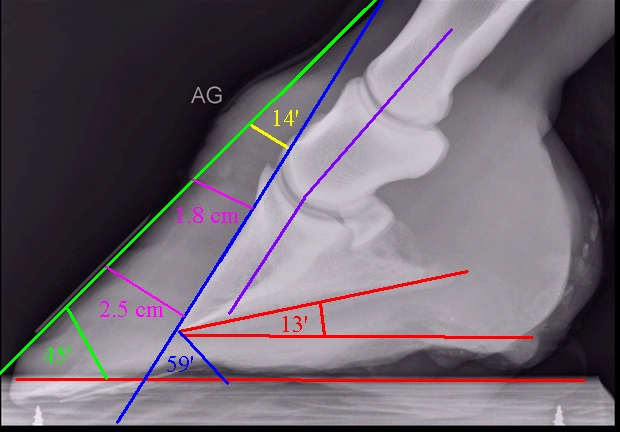
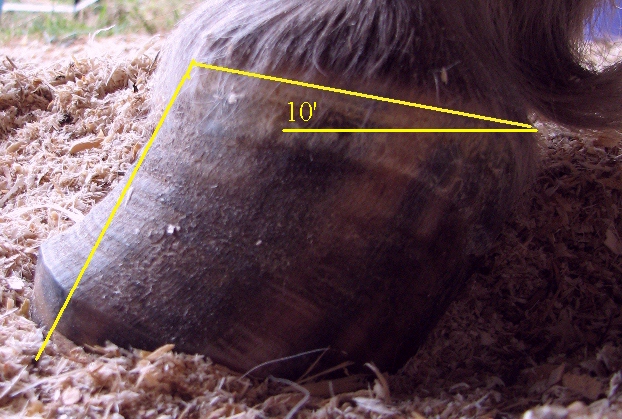
13' palmar & 14' dorsal rotation, laminar wedge
|
Abnormal heel growth

Change of angle, hoof rings

Stretched white line
|
Symptoms of chronic laminitis - rotation/sinkingRadiographs (x-rays) should always be taken when a horse has had, or is suspected of having had, laminitis. Many of the signs of chronic laminitis may not be seen until several weeks after laminar damage occurred, and not all of these signs will be seen - but the presence of any of these signs should be investigated.
See Chronic laminitis for more photos
|
Emergency treatment for laminitis
|

|

|
Management of laminitis
|

|
Prevent and monitor for laminitis
Prevent laminitis by ensuring your horse
Daily checks that can help early identification of laminitis:
- is not overweight,
- is regularly exercised (as long as feet are correctly aligned and stable),
- and if laminitis is a possibility, feed a low sugar/starch diet and restrict grass by using a muzzle, strip grazing or setting up a track, and allow grazing only when sugar levels are likely to be lowest - remember sun = sugar! If in doubt, don't graze! See www.safergrass.org for information about sugar levels in grass.
Daily checks that can help early identification of laminitis:
- Walk on hard ground e.g. concrete - does the stride shorten, does he/she seem at all "pottery"?
- Turn in a tight circle - normal or reluctant to turn/stiff behind?
- Digital pulses - normal?
- Regional fat pads - cresty neck, bulges in hollows above eyes, enlarged sheath, fat above tail? Hardening of neck crest or increase in any of these fat deposits can indicate imminent laminitis.
Frequently Asked Questions
Can a horse get laminitis in any foot?
Yes! With the exception of supporting limb laminitis which generally occurs in the foot opposite to the leg that is severely lame, laminitis (both SIRS and endocrine) is systemic (definition: affecting the entire body) and therefore the factors causing laminitis can affect any foot. Laminitis is often less severe in the hind limbs, but in some horses it is more severe in the hind limbs, or even on one side of the horse. It has been proposed that factors affecting which feet are more severely affected include weight bearing, hoof angle, hoof balance. More..
What's the prognosis for recovery from laminitis?
When the cause of the laminitis is identified and removed/treated, and the feet are supported and realigned at the earliest opportunity, the horse has a good chance of making a full recovery and returning to its previous work level. More..
Yes! With the exception of supporting limb laminitis which generally occurs in the foot opposite to the leg that is severely lame, laminitis (both SIRS and endocrine) is systemic (definition: affecting the entire body) and therefore the factors causing laminitis can affect any foot. Laminitis is often less severe in the hind limbs, but in some horses it is more severe in the hind limbs, or even on one side of the horse. It has been proposed that factors affecting which feet are more severely affected include weight bearing, hoof angle, hoof balance. More..
What's the prognosis for recovery from laminitis?
When the cause of the laminitis is identified and removed/treated, and the feet are supported and realigned at the earliest opportunity, the horse has a good chance of making a full recovery and returning to its previous work level. More..
Further information - websites:
No Laminitis! Symptoms of laminitis and emergency action
ECIRHorse Treatment of laminitis
Equine Laminitis Research Unit at the University of Queensland
Equine Laminitis - current concepts (2008) - Chris Pollitt
Equine Laminitis - managing pasture to reduce the risk - Katy Watts & Chris Pollitt
Information on the prevention and treatment of laminitis in horses and Katy Watts’ research into sugar/carbohydrate levels in grass and hay is available at the Safergrass.org website and Safergrass Yahoo group
The HORSE.com fact sheet: Laminitis
ECIRHorse Treatment of laminitis
Equine Laminitis Research Unit at the University of Queensland
Equine Laminitis - current concepts (2008) - Chris Pollitt
Equine Laminitis - managing pasture to reduce the risk - Katy Watts & Chris Pollitt
Information on the prevention and treatment of laminitis in horses and Katy Watts’ research into sugar/carbohydrate levels in grass and hay is available at the Safergrass.org website and Safergrass Yahoo group
The HORSE.com fact sheet: Laminitis
Laminitis Research
Research papers relating to laminitis, EMS and PPID are listed by date, subject and author under Research.
https://researchonline.rvc.ac.uk/id/eprint/11852/1/11852.pdf
Patterson-Kane JC, Karikoski NP, McGowan CM
Paradigm shifts in understanding equine laminitis
The Veterinary Journal Volume 231, January 2018, Pages 33-40
Pollard D, Wylie CE, Verheyen KLP, Newton JR
Assessment of horse owners' ability to recognise equine laminitis: A cross-sectional study of 93 veterinary diagnosed cases in Great Britain
Equine Vet J. 2017 Nov;49(6):759-766. doi: 10.1111/evj.12704. Epub 2017 Jul 3
See also: EVJ Podcast, No 21, Aug 2017 – Horse owners’ ability to recognise equine laminitis
A review of recent advances and current hypotheses on the pathogenesis of acute laminitis
A recently published paper by Lisa Katz and Simon Bailey outlines the current thinking that there are likely to be 3 distinct forms of laminitis - inflammatory (SIRS), endocrine and contralateral (supporting) limb laminitis, and suggests that there may be some interplay between the different forms - the full paper is available free online:
Katz LM, Bailey SR
A review of recent advances and current hypotheses on the pathogenesis of acute laminitis
Equine Veterinary Journal Volume 44, Issue 6, pages 752–761, November 2012
https://researchonline.rvc.ac.uk/id/eprint/11852/1/11852.pdf
Patterson-Kane JC, Karikoski NP, McGowan CM
Paradigm shifts in understanding equine laminitis
The Veterinary Journal Volume 231, January 2018, Pages 33-40
Pollard D, Wylie CE, Verheyen KLP, Newton JR
Assessment of horse owners' ability to recognise equine laminitis: A cross-sectional study of 93 veterinary diagnosed cases in Great Britain
Equine Vet J. 2017 Nov;49(6):759-766. doi: 10.1111/evj.12704. Epub 2017 Jul 3
See also: EVJ Podcast, No 21, Aug 2017 – Horse owners’ ability to recognise equine laminitis
A review of recent advances and current hypotheses on the pathogenesis of acute laminitis
A recently published paper by Lisa Katz and Simon Bailey outlines the current thinking that there are likely to be 3 distinct forms of laminitis - inflammatory (SIRS), endocrine and contralateral (supporting) limb laminitis, and suggests that there may be some interplay between the different forms - the full paper is available free online:
Katz LM, Bailey SR
A review of recent advances and current hypotheses on the pathogenesis of acute laminitis
Equine Veterinary Journal Volume 44, Issue 6, pages 752–761, November 2012
Useful resources for Laminitis
Laminitis webcasts and videos
Laminitis webcasts and videos
The Humble Hoof podcast with Dr Andrew Van Eps 11 Nov 2019
"In this episode, Dr. Andrew Van Eps delves into new research on laminitis and founder treatment, as well as the importance of prevention. In it, you will hear about the three causes of laminitis, and research into how to approach each cause. Prevention is better than "damage control," and implementing some changes in your horse's diet and lifestyle can make all the difference!"
"In this episode, Dr. Andrew Van Eps delves into new research on laminitis and founder treatment, as well as the importance of prevention. In it, you will hear about the three causes of laminitis, and research into how to approach each cause. Prevention is better than "damage control," and implementing some changes in your horse's diet and lifestyle can make all the difference!"