
Gas pocket/area of separation
Successful foot rehabilitations 1 solar penetration
Changes at the coronary band
Abscesses
Sinking/distal descent
Successful foot rehabilitations 1 solar penetration
Changes at the coronary band
Abscesses
Sinking/distal descent
Gas pocket/area of separation
Case 1. A horse developed laminitis on 15 December 2017. X-rays taken on 24 December 2017 showed areas of different shades of grey between the pedal bone and hoof wall, but no clear gas pocket/area of separation. 4 days later (28 December 2017) an thin line of separation was visible between the areas of different shades of grey. A month later (25 January 2018) there is a clear area of separation/gas pocket, that has already grown down since December. 2 months later (28 March 2018) the area of separation is wider and is significantly further down (the front of the pedal bone). By June (3 months later) the area of separation has almost grown out, and by December (6 months later) there are no signs of separation.




|
In March 2020 the horse was foot sore and more x-rays were taken. Areas of different shades of grey were seen on both left and right front feet. However, the horse soon became sound, and although further x-rays have not been taken, there has been no reason to suspect areas of separation.
|
|
Case 2. A mare developed sepsis-related laminitis after retaining the placenta following foaling.
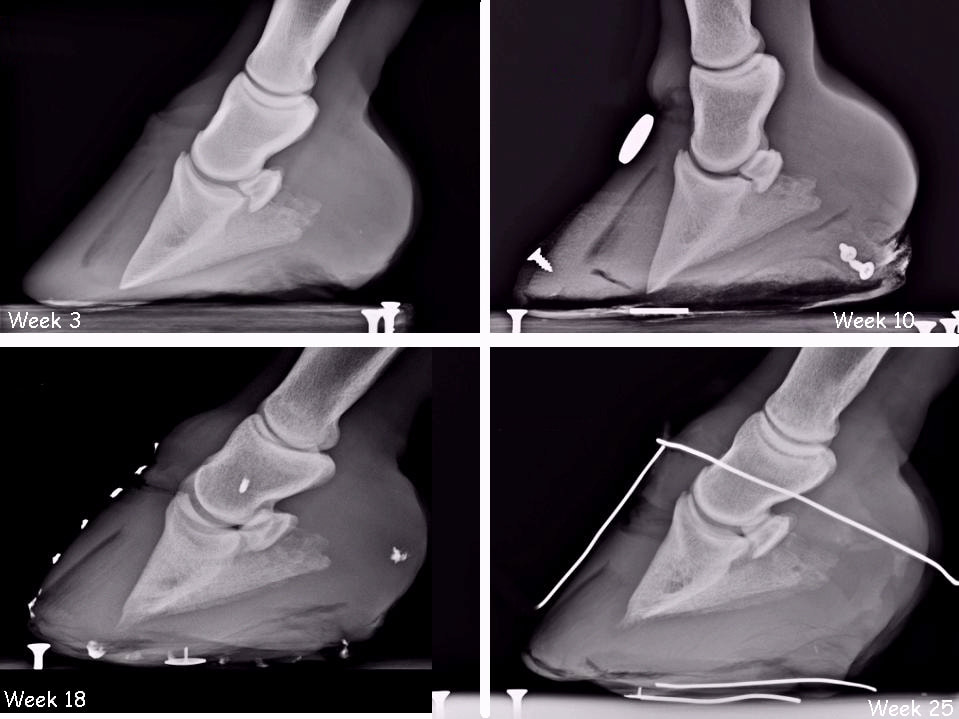
Left fore: initial x-rays 3 weeks after developing laminitis showed a significant area of separation on both front feet, which appeared more significant 7 weeks later, with signs of sub-solar abscessing (week 10). Realigning trimming was not started until week 12, by which time the pedal bones on both front feet had penetrated the sole. Conditions and trim frequency were not ideal during the mare's rehabilitation, but nonetheless within 6 weeks of starting realigning trimming the feet were starting to be realigned with increased sole depth, and the area of separation was growing down and out, and was removed during the trim following the week 25 x-rays, at which point the feet were basically realigned.
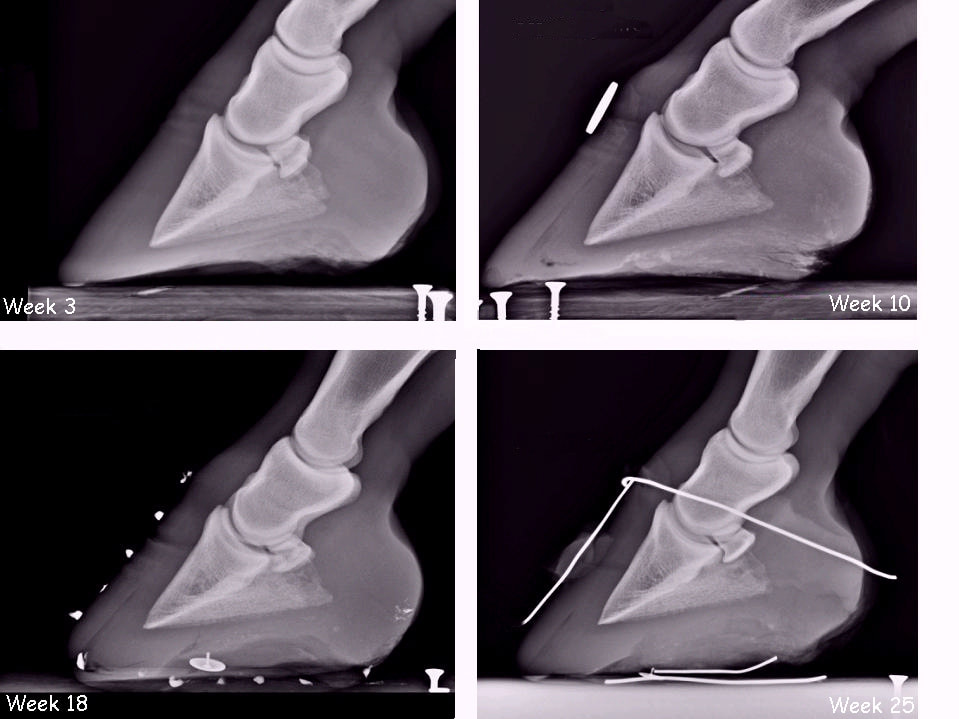
Left hind: initial x-rays 3 weeks after developing laminitis showed no obvious area of separation on either hind foot, but 7 weeks later a dark line of separation can be seen, which grew down and out.
Successful foot rehabilitations - 1 solar penetration





Changes at the coronary band
In After The Crash - Lessons from Chronic Laminitis, Professor Chris Pollitt writes:
"Coronary band changes.
When the majority of the lamellar attachments fail, as they do in severe cases (sinkers), P3 descends deeply into the hoof capsule, taking with it the attached coronary band connective tissue. This creates a deficit in the coronary band and the sharp edge of the proximal hoof wall becomes palpable with a finger. Initially the deficit may be palpable only dorsally (the front of the foot), over the extensor process of P3. If it extends around the coronary band to the quarters and heels, the prognosis is grave, as this is an indication that most of the lamellar attachment apparatus is destroyed. Sometimes the skin may separate at the hairline of the coronary band and exude serum."
"Coronary band changes.
When the majority of the lamellar attachments fail, as they do in severe cases (sinkers), P3 descends deeply into the hoof capsule, taking with it the attached coronary band connective tissue. This creates a deficit in the coronary band and the sharp edge of the proximal hoof wall becomes palpable with a finger. Initially the deficit may be palpable only dorsally (the front of the foot), over the extensor process of P3. If it extends around the coronary band to the quarters and heels, the prognosis is grave, as this is an indication that most of the lamellar attachment apparatus is destroyed. Sometimes the skin may separate at the hairline of the coronary band and exude serum."
Case 1. A horse became lame in June, laminitis wasn't diagnosed until July, x-rays taken, heart bars fitted 13 July. 26 August became severely lame, x-rays showed significant rotation both fronts, heart bars remained on with gel insert, apparently no attempt to realign rotation. Horse had been asked to walk and turn by vet, vet reported to be "baffled". End September TLS involved, horse severely lame on LF with heel held off the ground. New vet practice took over end September, shoes removed, x-rays - showed significant sinking, compression (?) at coronary band, significant dorsal and palmar rotation, area of separation along full length of laminae, inadequate sole depth.

10 July - the coronary band looked slightly bumpy. There was reasonable sole depth.
|
27 August - the coronary band was starting to look compressed/tight. There was dorsal rotation and significant palmar rotation that needed to be corrected urgently.
|

27 August - a darker line can be seen towards the top of P2 which was presumably the coronary band
|

29 September - the coronary band was starting to look quite abnormal - tight/compressed and ridged.
A large area of separation (gas line) was opening up, there was significant dorsal and palmar rotation that needed to be corrected urgently.
|

06 October before trimming. The horse was lifting the heel off the ground most of the time.
|

06 October after a small trim.
|

10 November. There was considerable swelling above the coronary band, compression/disruption at the coronary band, the horse was not weighting the heel.
|

10 November. 0DP view but with the horse not weighting the heel. There was considerable swelling above the coronary band and compression/disruption at the coronary band.
|

10 November. The situation suddenly deteriorated, the heel was off the ground all the time, the foot was cold....
|

10 November. The coronary band had become sore and was weeping, and there was considerable swelling above the coronary band. Despite antibiotics and pain relief, expert assessment was that there was likely to be infection around the coronary band and loss of perfusion, and the horse was sadly PTS.
|
Abscesses
Horse 1



Sinking/distal descent
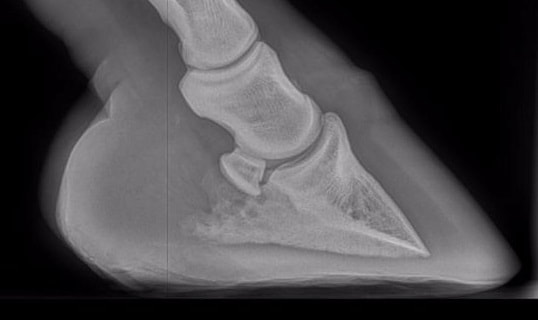
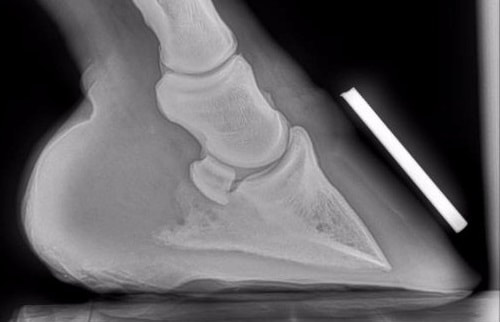
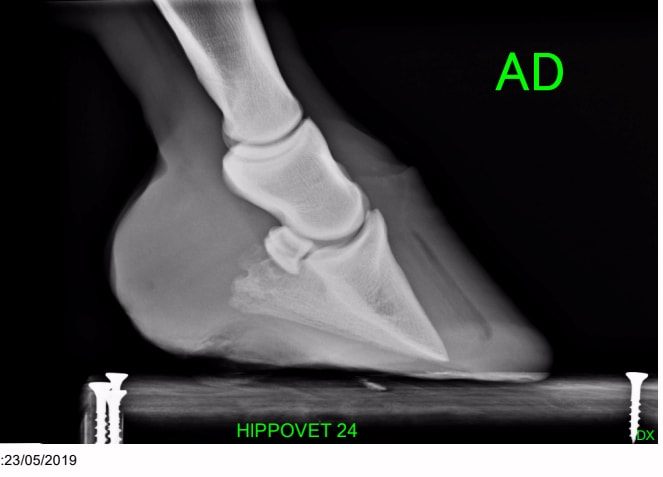
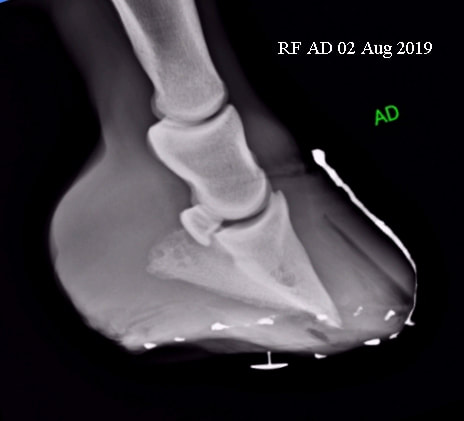
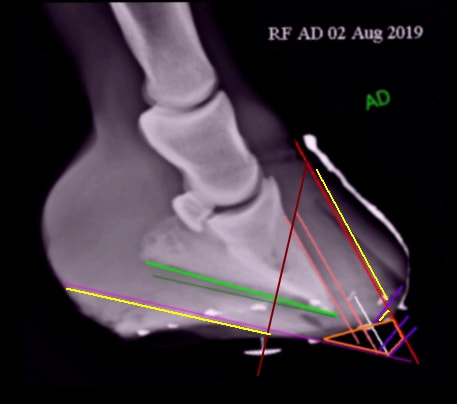
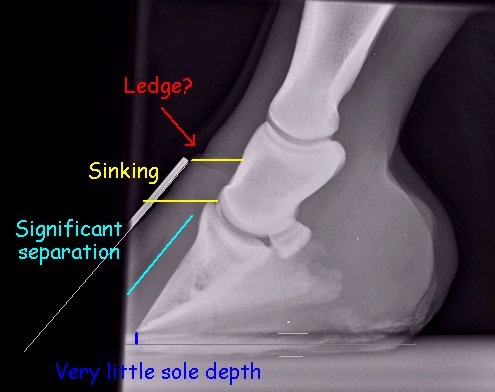
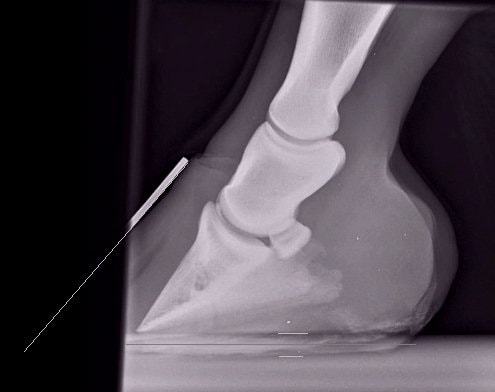
1. This horse appeared to have an acute inflammatory disease (the disease was never diagnosed but blood tests suggested significant inflammation - Lyme disease or perhaps toxicity were suggested as possible causes), and his laminitis presented as a sepsis-related laminitis, with sinking and lack of sole depth in all 4 feet.
Although there are no pre-laminitis x-rays for comparison, the clinical signs suggested that there was sudden significant sinking of the pedal bone into the hoof capsule, reducing sole depth.
Red - a ledge or ridge can be seen at the coronary band - this could be palpated on the foot.
Yellow - sinking/distal descent distance.
Turquoise - a large gas pocket/area of separation was seen between the pedal bone and the toe wall.
Dark blue - there was very little sole depth.
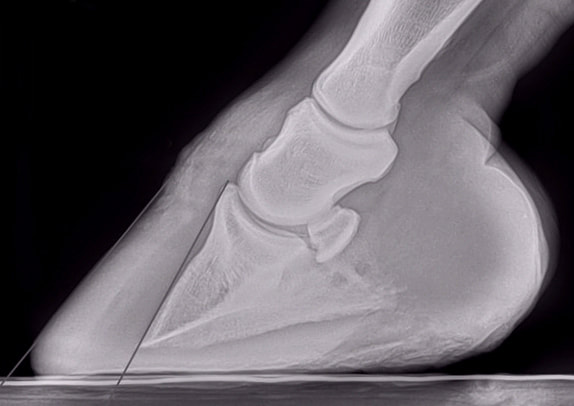
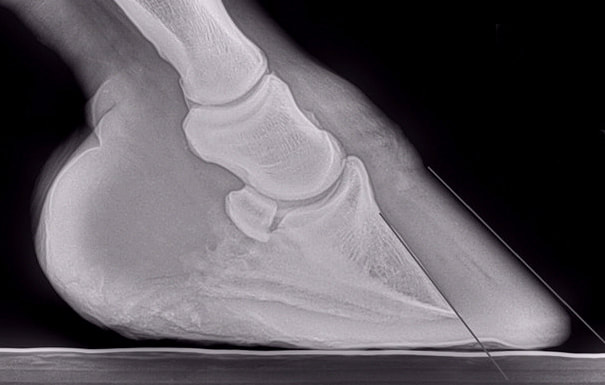
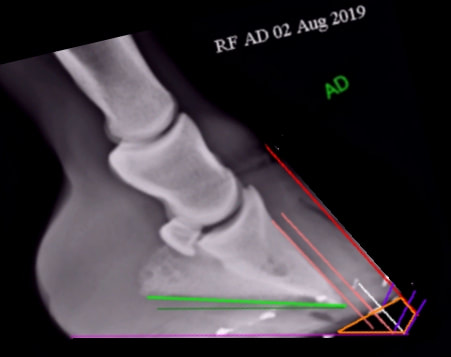
Although there are no pre-laminitis x-rays for comparison, the clinical signs suggested that there was sudden significant sinking of the pedal bone into the hoof capsule, reducing sole depth.
Red - a ledge or ridge can be seen at the coronary band - this could be palpated on the foot.
Yellow - sinking/distal descent distance.
Turquoise - a large gas pocket/area of separation was seen between the pedal bone and the toe wall.
Dark blue - there was very little sole depth.
|
|