
It was Nutmeg's owner Laurie's birthday this week, and she posted to say that:"The best present I have had is this...
Posted by The Laminitis Site on Friday, 17 April 2015
|
0 Comments
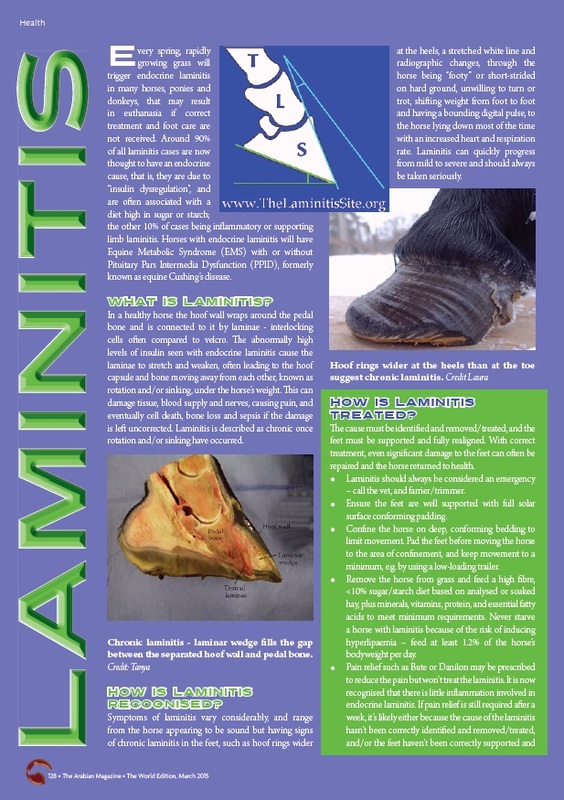 The Laminitis Site's article on laminitis that appeared in The Arabian Magazine March 2015 - click on the image to read the full article The first in a series of articles about laminitis written by The Laminitis Site was published in The Arabian Magazine's March 2015 edition.
More news can be found on our Facebook page.
Articles Recently published research now has its own page under Research. For future and past conferences see Conferences.
The Laminitis Site is appealing for donations of new or used hoof boots for the Boot Bank it is setting up.
The dexamethasone suppression test is no longer suggested - hurray!
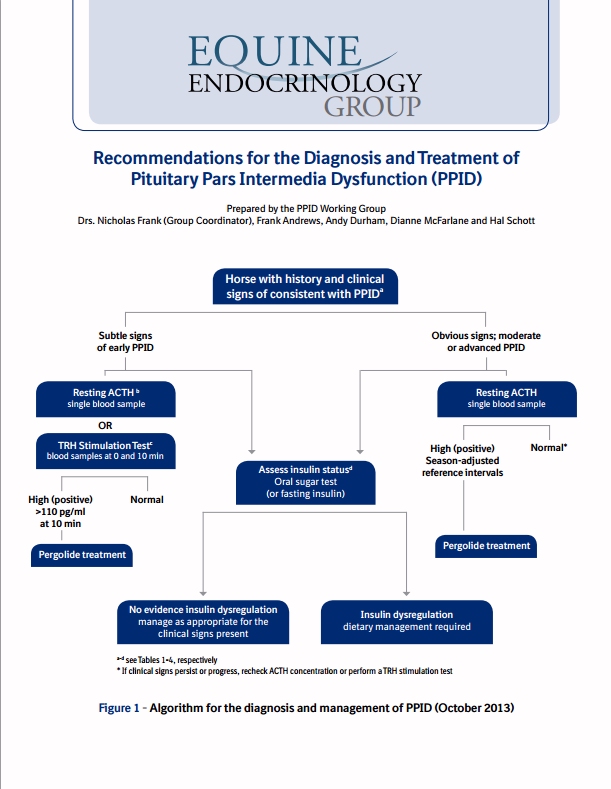
As in the earlier guidelines, clinical symptoms of PPID are given split into early: decreased athletic performance, change in attitude/lethargy, delayed haircoat shedding, regional hairiness (hypertrichosis), change in body shape, regional adiposity (fat pads), laminitis; and advanced: lethargy, all over hairiness (hypertrichosis), failure to shed haircoat, muscle loss, pot belly, abnormal sweating (increased or decreased), increased drinking/urination, recurrent infections, regional adiposity, loss of seasons/infertility, laminitis, raised glucose levels (hyperglycaemia), neurological symptoms/blindness. Instructions are given for preparing the blood samples for ACTH testing, and the warning included that freezing samples without prior centrifugation can cause falsely high results. Interestingly, Liphook's cut-offs for resting ACTH are given as 47 pg/ml Aug-Oct, 29 pg/ml rest of year (using Immulite CIA), and Cornell's (also using CIA?) as 35 pg/ml Nov-July and 100 pg/ml mid Aug-mid Oct, although this is qualified as needing further research. No mention is made of the "grey area" that Andy Durham and David Rendle of Liphook have talked about of 20 - 40 pg/ml Nov-July (and therefore it is assumed approx. 10 pg/ml either side of 47 Aug-Oct), when further testing is recommended - although the Recommendations do suggest further testing for results near the cut-off. The suggested cut-offs for the TRH stimulation of ACTH have been raised slightly - now 110 pg/ml exactly 10 minutes after TRH administration and 65 pg/ml 30 minutes after TRH administration. The TRH stimulation of ACTH is currently not validated for use between July and November (inclusive), and further research is ongoing to verify the above suggested cut-offs. As part of the workup for a diagnosis of PPID, it is suggested that insulin status is assessed (and glucose). The EEG now suggests using the oral sugar test (OST) as the first choice for assessing insulin status. However, if the owner is concerned about the OST increasing laminitis risk, a fasting insulin concentration should be measured first and if normal, then the OST should be carried out (this would involve 2 vet visits). Liphook have confirmed that they are happy for owners in the UK to use Karo Light corn syrup, i.e. carry out the OST rather than the in-feed glucose test which uses a much larger amount of glucose - Karo Light corn syrup can be purchased from Amazon in the UK. Owners worry about fasting their horse overnight for the fasting insulin test - the Recommendations suggest leaving one flake of hay at 10 pm and collecting blood the next morning. It is pointed out that a normal fasting insulin result is not diagnostically significant - only an above normal insulin result is significant. A list of potential tests (for PPID) that are not commercially available is given - if only they were available now, but hopefully in the future! They include (as you would expect): Alpha-MSH, bioactive ACTH, POMC, beta-endorphin and CLIP. TLS has been saying for some time that the best test for PPID has to be to measure as many of the affected hormones as possible... And the list of tests no longer recommended for PPID diagnosis includes anything to do with cortisol! It is now recommended that pergolide/Prascend is "introduced gradually by giving partial doses for the first four days or by administering half the dose morning and evening." Excellent! NB if you are in the UK, your vet can ask BI for a pill splitter - see Splitting Prascend tablets. Suggestions are given for the response you might expect to see to treatment with pergolide/Prascend: Within 30 days - improved attitude, decreased drinking/urination, increased activity and reduced hyperglycaemia. Anything from 1 to 12 months - improvements in haircoat abnormalities, less of a pot-bellied appearance, fewer infections, improved topline, less laminitis. Treatment should be continued for at least 2 months before conclusions can be made about changes to symptoms. Retesting after 30 days of treatment is suggested to assess response to treatment. If test results are normal the dose is not increased. If test results remain above normal but clinical symptoms have improved, the dose can either remain the same or be increased. If test results remain above normal and clinical symptoms have not improved, the dose of pergolide/Prascend should be increased (and possibly the addition of cyproheptadine considered).
"Pour favoriser le diagnostic des chevaux atteints, Boehringer Ingelheim soutient une campagne de dépistage en offrant un dosage ACTH pour les cas suspects." Boehringer Ingelheim are offering free ACTH testing for horses in France through VetAgro, the vet school at Lyon. The free test is offered for horses over the age of 10, that have presented with laminitis with no obvious cause. Given that probably over 90% of laminitis cases are endocrine, which will be EMS and/or PPID, this will be most first time cases of laminitis. Horses under 10 can get PPID too, so it's a shame that the free test excludes younger horses. The protocol calls for blood to be collected into EDTA (purple topped tube), centrifuged within 2 hours, chilled until despatch to the lab or frozen before despatch. As ACTH levels decline in unchilled blood, TLS recommends freezing the samples before despatch (but the blood must be separated by centrifuge, not by gravity, before the plasma is frozen, otherwise falsely high ACTH results are likely to be seen). More information: Free test offer Dysfonction Par Intermedia (maladie de Cushing) Cheval Protocol NB insulin should also be tested in all horses with endocrine laminitis. ACTH is diagnostic for PPID, but insulin is suggestive of laminitis risk. Liphook Equine Hospital Laboratory Newsletter winter 2012/13
Frank Duncombe Laboratory in Normandy (France) is now testing ACTH (EDTA) and insulin (serum), presumably using a similar protocol to Liphook Equine Hospital. Prices we've been told are
ACTH: 37,36€ TTC Insulin: 19,48 € TTC Laboratoire Frank Duncombe, 1 Route de Rosel, Saint Contest, 14053 Caen T: 02 31 47 19 50 email: lfd-sante@calvados.fr |
News
What's new in research New Dengie Laminitis Brochure uses TLS photos WHW new laminitis leaflet2020 Global Equine Endocrine Symposium proceedings Articles about feet December 2019 Autumn Laminitis with Danica Pollard Free ACTH Testing Do all IR/EMS horses have laminitis? Clinical signs of PPID may vary with location Velagliflozin - preventative treatment for endocrinopathic laminitis? USEF allows pergolide to be taken by competing horses Pergolide molasses-flavoured paste available in UK NEHS 2018 Risk factors for EMS/Endocrinopathic Laminitis Seasonal rise in pituitary hormonesPPID - weekly ACTH cutoffs now being used Sole Support Do you CARE about laminitis? Pituitary Pars Intermedia Dysfunction - The Arabian Magazine EMS & Insulin Dysregulation - The Arabian Magazine Laminitis and the Feet - The Arabian Magazine The Arabian Magazine Laminitis article Paddock Paradise in French New EEG Recommendations for the diagnosis and treatment of PPID Archives
February 2024
Categories |







 RSS Feed
RSS Feed